At the end of January 2018, I attended the Hanson Wade Tumor Models Conference in San Francisco. I had the opportunity to co-present a workshop discussing The Jackson Laboratory’s Onco-Hu® Mouse Models as novel immuno-oncology platforms to test the efficacy of check-point inhibitor molecules. Aside from being able to combine two of my favorite topics – science education and oncology – I surveyed the various strategies researchers worldwide are using to develop cancer immunotherapies. While numerous immune cell types interact with tumor cells, T cells remain a primary focus for therapy.
Given that mouse biology doesn’t always predictably model human biology, how are some researchers developing T cell-based immunotherapies in the preclinical space?
Classic syngeneic tumor models allow the study of endogenous T cell function
Tumors that spontaneously arise or are experimentally induced in a mouse can sometimes be isolated and propagated in vitro. When these cell lines (such as CT26 colon carcinoma or 4T1 mammary carcinoma cell lines) are injected back into the compatible inbred mouse strain of origin (BALB/cJ in this case), these syngeneic models allow the study of endogenous T cell function in fully immune competent mice.
- University of Chicago researchers used the C57BL/6-derived B16F10 melanoma cell line to investigate the role of the microbiome in immunotherapy. Anti-PD-L1 therapy generated stronger tumor-specific T cell responses and intratumoral CD8+ T cell accumulation when the cells were implanted in the C57BL/6J mouse substrain from The Jackson Laboratory (JAX) compared to the C57BL/6Tac mouse substrain from Taconic Farms. Members of the genus Bifidobacterium, found in higher composition in the microbiome of the JAX mice, exerted these anti-tumor effects.
- Mariathasan and colleagues selected the BALB/c-derived EMT6 mammary carcinoma cell line to study tumors that do not respond to anti-PD-L1 therapy. They found that co-administration of anti-PD-L1 with anti-TGFβ, which targeted tumor stromal cells, allowed for better T cell infiltration into the tumor and improved tumor regression.
Basic T cell immuno-oncology and proof-of-concept studies are possible using syngeneics, but may lack translatability to human-specific molecules. However, translatability will likely be improved in the near future with the advent of CRISPR/cas9 technology to quickly generate mouse models with human-specific variant molecules (JAX CRISPR/cas9 Precision Mouse Models Service).
Immunodeficient mice permit the study of human T cells and human cancers in vivo
Permissive immunodeficient mouse strains, which lack the ability to mount an immune response, can be engrafted with tissues from human donors to generate human-specific therapies. Some very highly sophisticated models include co-engraftment of both human immune cells and human cancer cell lines or Patient-Derived Xenografts (PDX) (JAX Onco-Hu® Models).
- Chimeric Antigen Receptors (CARs) have been used clinically to treat leukemia with success. However, the current versions can elicit unintended inflammatory immune reactions, because they contain fragments of mouse origin. To address this, Sommermeyer and colleagues employed the severely immunodeficient NSG mouse strain to test fully human CD19 chimeric antigen receptors (CARs) against a human leukemia. They successfully showed reductions in the immunogenicity.
- Researchers at Merck chose both syngeneic models and NSG mice humanized with CD34+ hematopoietic cells to test the efficacy of anti-GITR on a human melanoma cell line. Treatment with anti-GITR antibody reduced the Treg population and activity within the spleen and tumor, allowing CD4+ and CD8+ T cells to increase production of antitumor effector cytokines.
Immune system humanization continues to be improved with the addition of transgenic human cytokines, such as in NSG-SGM3 mice that express human IL3, CSF2, and KITLG. Additionally, when NSG mice are engineered to express human MHC molecules, such as NSG HLA-A2, and are paired with matched PDX and CD34+ cells, the humanized T cells can become appropriately HLA restricted.
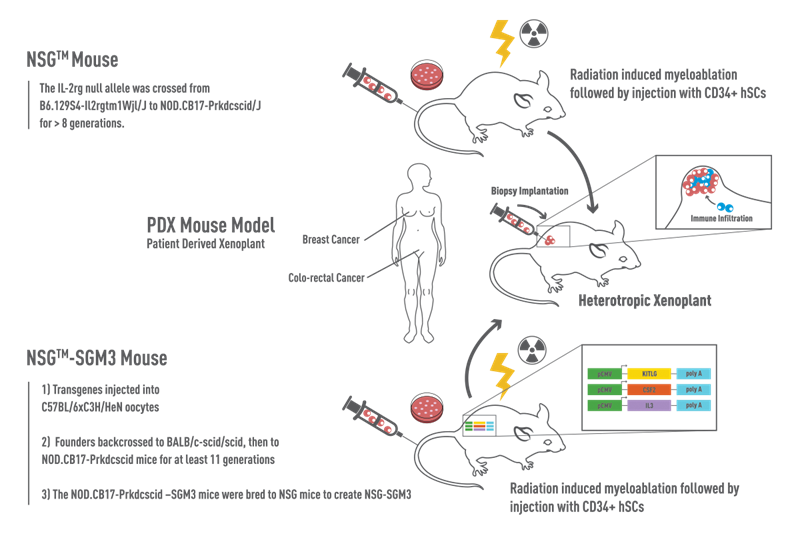
Figure 1: NSG vs NSG-SGM3 Mice. NSG™ mice (NOD.Cg-Prkdcscid Il2rgtm1Wjl/SzJ, 005557) are devoid of mature B, T, and NK cells. NSG™-SGM3 (NOD.Cg-Prkdcscid Il2rgtm1Wjl Tg(CMV-IL3,CSF2,KITLG)1Eav/MloySzJ, 013062) are NSG™ mice that contain transgenes expressing human Stem Cell Factor (KITLG), GM-CSF (CSF2), and IL-3. Recipient mice were irradiated at 3-4 weeks of age and engrafted with human-cord-blood derived CD34+ hematopoietic stem cells. Prior to co-engraftment of human tumors, mice are validated for human multilineage engraftment and establishment of human immunity.
Ex vivo models facilitate quick compound screening or genomics analysis
Patient-to-patient variability and intratumor variability can be modeled using clinically relevant patient-derived tumor tissues either in vivo or ex vivo. Scalability is a primary advantage of ex vivo modeling, including screening compound libraries on a large number of diverse samples. In addition, primary tissues can be cultured on a short term basis and contain autologous stroma and passenger immune cells that would be lost if the tissues were passaged in vivo. Using a bank of primary tumor tissues, genomics and bioinformatics analyses may allow broader generalizations about cancer signatures.
At the conference I was struck by the wide variety of in vivo and ex vivo models that are helping to develop better, more targeted cancer therapies. One thing was clear: models are approximations, and multiple models are needed to adequately understand and treat a disease. Certainly with a disease as complex and heterogeneous as cancer, there is no exception to this rule.